Testimonials and Success Stories-Inspiring Journeys to Better Heart Health
Our Success Stories in High Risk Situations In Cardiac Surgery
1. 52yrs Male was admitted with Severe Calcific aortic stenosis with LVF. His heart function on 2D Echo was 25% with features of pulmonary oedema. He was admitted stabilized and decongested. His angiography revealed a diagonal branch having 50% stenosis. After 2 weeks of stabilization he was taken up high risk aortic valve replacement. His Echo followed by CT scan showed grossly dilated aortic root of (5.5 cm). It was debated whether to change only valve or replace the aortic root with valved conduit. Since he was very sick it was decided to go ahead prepared for root replacement but if aortic walls were preserved only aortic valve will be changed. Under standard cardiopulmonary bypass and cardioplegic arrest aortic valve are changed with 21mm St. Jude valve. Post operatively he behaved well and remained stable and was discharged on 8th POD. In the follow up his heart function has returned back to normal.
2. A 59yrs old male was admitted with dilated ischemic cardiomyopathy with EF of 20% and severe Mitral Regurgitation, acute LVF and NIDDM. With renal dysfunction. He was put on IABP pre – operatively and CAG revealed diffuse Triple Vessel Disease. In spite of IABP and Inotropic support patient remained in LVF and blood counts were high. He was on heavy antibiotic. It was decided to intervene surgically and CABG with MVR was done. Three vein grafts were put and mitral valve changed with 27mm St. Jude valve. Post operatively patient improved fast and extubated 3rd POD and IABP removed 5th POD and was discharge on 13th day. His follow up showed improvement in his heart function to 38%.
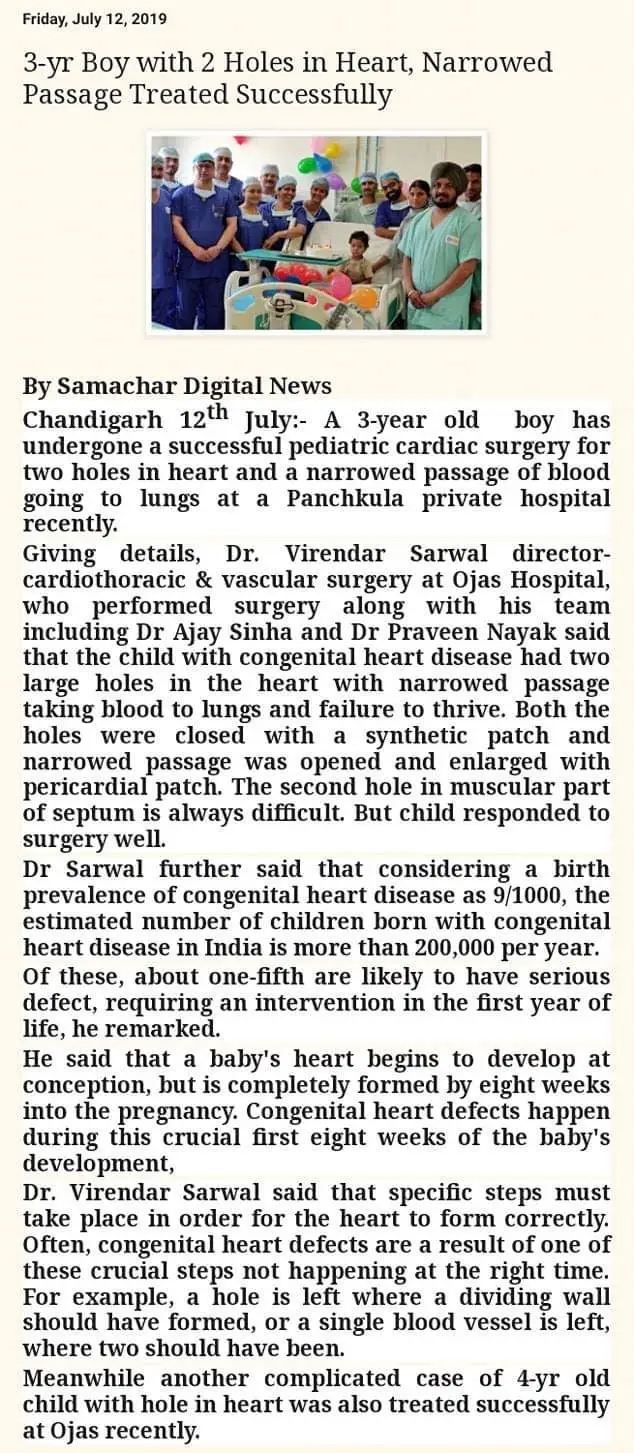
3. A 4yrs old female presented to us as blue baby since birth and on investigation was found to be having classical pentalogy of fallot but with very small pulmonary arteries and failure to grow. At 4yrs her weight was 8kgs only. Both the pulmonary arteries were small and made her high risk for surgery but was again treated and operated and her hole in heart was cleared with Dacron patch and pulmonary arteries enlarged with a pericardium patch across the outflow track of right ventricle. ASD was closed and post -op she was electively ventilated for 72hrs and then extubated recovered and discharged well after 8 days.
4. A 59yrs old male was brought to hospital with acute anterolateral MI with thrombus in LAD Ostea, acute pulmonary oedema and EF of 40%. He was immediately taken up for angiography which showed left main stenosis with critical Triple Vessel Disease. He was out on IABP as he was not maintaining pressure and was having arrhythmias. With in 3hrs of reaching hospital he was taken into Operation Room for CABG and 4 grafts were put in on him on beating heart. He improved and remained stable in post operative period was extubated on 1st POD on discharged on 8th day on good condition. Post-op Echo shows normal heart function.
5. Ojas Hospital, Mohali helps save life of a critically ill Poor Patient with LifeSaving Heart Surgery A 31 years old gentleman presented to Ojas hospital, Mohali with acute breath lessness, vomiting for last four days. He was having this problem for the last one years and was in the follow up of another hospital where he was diagnosed to be having leakage of both the major valves of heart following fever and cough with expectation.For the last four days even he was not able to lie down flat in the bed because of severe breathlessness and heart failure. His liver was severely enlarged and his echo cardiograph showed a dilated heart with severe leakage of one valve and moderate leakage in the other with a hole in the leaflet of one of the valve (aortic valve) with sign of vegetation on it. He was on medical treatment with the other Institute before getting admitted under Dr Anurag Sharma Sr. Consultant Cardiology.He was put on decongestive treatment and echo here showed ruptured leaflet of aortic valve with severe leakage and liver was congested with fluid in the lungs. After two days of his treatment he was planned for valve replacement surgery .As he started responding to medical treatment he was shifted to the ward from ICU but as he was poor and was not able to afford surgical treatment which was required urgently for him, Ojas Hospital, Mohali decided to arrange finance for him through Max India foundation and they very graciously arranged 1.2 lakh for him for the surgery withfurther contribution from the hospital. But a day later his condition worsened and he went into shock state because of congestive heart failure with his heartrate dropped to 30/per mint. His urine output also dropped and he went intorenal shutdown. He was shifted back to ICU and had to be put on ventilator asan emergency and drugs started to maintain his B.P. Next day his condition improved and he started stabilizing under Doctor Anurag Sharma and this team.With great efforts again he stabilized and was removed from the ventilator but still wason medication to support his heart. After five days of aggressive treatment he was weaned of from all drugs but his liver functions were still deranged. As there was no other alternative he was planned for emergency surgery requiring replacement of both the valves as his echo showed second valve also leaking severely after this episode.The case was renewed by Dr. Virendar Sarwal, In charge of Cardiac Surgery and his team and a request for more funds was made to Max India foundation and additional money was sanctioned for him. After four days of more stabilization and with improvement in liver functions he was taken for surgery with a plan to change the ruptured aortic valve and repair of the mitral valve. On Trans Esophageal echo cardio graphin O.T it was observed that the leakage in mitral valve is due to jet of leakage of the aortic valve and as such mitral valve was normal. Other factor for the leakage of this valve was dilated leftchamber ofthe heart. So it was plannedthat with the change of aortic valve the leakage of mitral will go down becausethe jet from aortic valve will disappear and dilatation of chamber will also godown. Under cardiopulmonary bypass his aortic valve was changed with a 22 sizedmechanical valve by a team composing ofDr.Virendar Sarwal, Incharge dept. of CTVS, Dr.Ajay Sinha, CardiacAnesthesia,Dr. Aratatran Nahak , Dr Goswami, Dr DeepakOberoi,and Dr Rajit and after coming off CPB, TEE was doneagain which showed disappearance of the leakage of the other valve.He wasshifted to ICU with moderate inotropics support and was weaned off fromventilator next day. He progressed very well in his post operative period andwas discharge on the 5th day from the hospital in a very stablecondition. On firstfollow up he isdoing very well back to normal life after about a month of hospitalization andstormy course which could have been life threatening for him. Thanks to theuntiring efforts of the whole team and a big help from Max India Foundation heis alive today.
6. Yes discharged 2days back a ticklish case of CABG for a patient who was taken for angioplasty to right side artery which dissected and created an MI. Not only that the guide wire got stuck in the false lumen and cardiologist while pulling it back broke it down in midway in descending aorta. After stabilization took him for CABG and on opening up it came out to be porcelain Aorta and it was impossible to clamp it. So gave up the idea of pulling out the wire by going on pump. Did a 4 graft offpump CABG by doing 2 proximal to Aorta with Enclose device with difficulty and 3rd proximal was piggy bagged on the other. Did well in the post op period but still keep wondering why he was at all taken up for angioplasty with so much calcium around.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}